






患癌母亲寻子26年抱憾离世,儿子竟是微信好友

甲状腺结节、甲状腺肿……微波消融术“一针”搞定!

6公分胰腺癌,纳米刀消融术精准击破
卵巢小细胞癌患者――我要活着,更要快乐并美美地活着

手术+介入治疗,胃癌患者锦旗相送表心意

纳米刀被《人民日报》报道!位于“第二肝门”的肿瘤无法热消融,

Nasir的故事
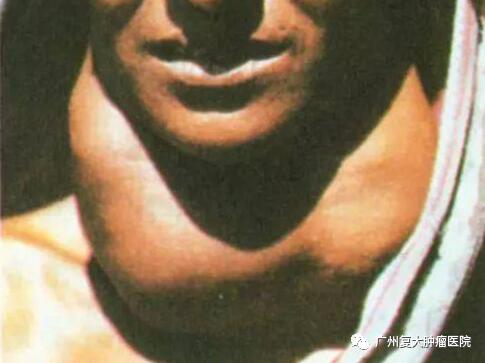
压在脖子上的重担――结节性甲状腺肿

您当前的位置: > 专家阵容 >
- 全网发布:01-16 11:55 发表者:广州复大肿瘤医院
哈森(HAMOOD MOHAMMED ABDULRAHMAN AL-KHASHEB)
姓名: 哈森(HAMOOD MOHAMMED ABDULRAHMAN AL-KHASHEB)

出生日期:1973年1月1日
性别:男 国籍:也门
外语水平: 精通英语 学位:医学博士
擅长领域:肿瘤外科、普外科
教育背景:
2002年9月-2006年6月,在中山大学主修研究生培养计划规定的全部课程,硕士研究生毕业。
2008年9月-2014年6月,在中山大学主修博士研究生培养计划规定的全部课程,以《原发性肝癌的根治性手术后规则局部门脉化疗的研究》论文顺利完成博士研究生毕业。
毕业于中山大学医学院,也门共和国外科学会委员、ASC亚洲冷冻治疗学会委员。从医15年,拥有丰富的疑难疾病诊断和大量手术治疗的临床经验,长期从事胰腺癌、肝癌、肺癌、乳腺癌、肾癌、甲状腺癌、腹腔肿瘤的外科手术和综合治疗,在氩氦刀冷冻治疗肝癌、甲状腺、颈部肿块、乳腺癌及经皮冷冻胰腺癌方面拥有丰富的经验。
个人研究
肝癌治疗常用的方法有:肝切除术、肝动脉栓塞化疗(TACE)、局部消瘤减瘤治疗(微波消瘤减瘤、射频消瘤减瘤、无水酒精注射)、靶点导向药物治疗、生物免疫治疗等。对于早期肝癌病人而言,手术切除是首选的治疗方法,部分病人可以获得长期生存。但是肝癌术后复发是影响肝癌手术效果的重要因素,也是最终导致病人死亡的重要原因之一。大肝癌术后5年复发率高达80%,小肝癌为40%~50%,最早的在术后2个月复发,复发高峰在术后1~2年。
肝癌切除术后复发的来源有两种:1.肝硬化的基础上出现新的癌灶,肝内复发灶为多发的而无血管侵犯的属于非同步多中心癌变的一个复发途径。2.肝内播散有血管侵犯的最重的复发进展期途径门静脉,肝静脉分支和主干形成癌栓,引起肝内多发转移最常见,肝硬化多见。
与其它肿瘤相比,肝癌的术后复发仍然缺乏有效的预防方法,应用的各种方法效果也并不肯定,同一种方法在不同的报道中可能会得出不同甚至截然相反的结论。常用的方法有术后辅助化疗:主要包括全身化疗和区域性化疗。全身化疗由于单药缓解率低,副作用大,在国外已经基本放弃应用。而靶点导向性药物如索拉非尼虽然证实其对肝癌的治疗效果,但是由于其昂贵的价格又极大的限制了其应用。
区域性化疗包括肝动脉给药和门静脉给药,由于这两种方式均是通过肝脏局部给药,药物浓度可以达到全身给药时的数百倍,提高了化疗效果而且降低了化疗药物引起的全身性不良反应,因此在临床上得到了广泛的应用。术后经股动脉穿刺肝动脉栓塞化疗(TACE)广泛的用于肝癌复发的预防性化疗,但是对其效果国内外仍然存在争议。有研究表明,原发性肝癌切除术后联合肝动脉栓塞和门静脉化疗有助于降低复发率,提高5年生存率。门静脉化疗的途径有两条:一是在肝癌切除手术中,从胃网膜右静脉插管至门静脉主干,然后连接注射药囊(俗称“化疗泵”)并埋置于皮下,术后经药囊注入化疗药物。二是术后在B超引导下,经过皮肤和肝脏穿刺门静脉的肝内分支,将导管插入门静脉主干,然后连接48小时持续输液泵注入化疗药物。
前者的优点在于:与手术同期埋入化疗导管,不需术后反复穿刺门静脉,病人痛苦小。缺点是:(1)导管长期留置于门静脉内,有引发门静脉血栓形成的危险。(2)导管留置时间过长容易出现堵塞,导致无法继续注药。(3)局部皮下有异物感。药囊与导管连接处可能出现松脱,导致化疗药物外溢于皮下组织,引起局部组织炎症、甚至坏死。后者的优点有:导管不需要长期留置于门静脉内,极少引起门静脉血栓形成和出现导管堵塞及药液外渗的现象。但该方法亦存在以下一些缺点:(1)需要反复多次穿刺肝内的门静脉分支,而且随着穿刺次数的增加,穿刺点处的门静脉壁由于反复机械性损伤导致增厚,引起管腔变细,导致穿刺成功率下降。(2)经皮经肝穿刺可出现误伤胆道,引起胆汁渗漏,严重时出现胆汁性腹膜炎。若凝血功能异常,拔出导管后,穿刺点出血不易自凝,导致腹腔出血。
在本组研究中,规则门静脉化疗组118例患者共完成超声引导下经皮经肝门静脉穿刺置管化疗526例次,共发生穿刺操作相关性并发症6例次,并发症发生率为(11.79%),其中包括肝包膜下出血1例(1/526,1.9‰),胆汁漏2例(2/526,3.8‰),门静脉血栓形成1例(1/526,1.9‰),导管相关性感染1例(1/526,1.9‰),导管脱落1例(1/526,1.9‰),所有并发症经保守治疗后均痊愈,未有致死性并发症。因此,我们认为该操作的安全性较高,适合临床大规模应用。
而在疗效方面,临床治疗组和实验对照组的2年复发率和总体复发率分别为21.2%VS37.2%(P<0.05),45.7%VS67.3%(P<0.05);临床治疗组和实验对照组术后2年生存率和总体生存率分别为83.1%VS69.8%(P<0.05),59.3%VS39.5%(P<0.05)门静脉化疗组和对照组术后中位生存时间分别为1500天VS1136天(P<0.05)。以上数据表明,术后规则的门静脉化疗可以有效降低术后肝癌复发率,延长病人生存时间。
我们的研究结果初步显示对于早中期的原发性肝癌患者,在行根治性手术后给予规则的超声引导下经皮经肝门静脉穿刺化疗是一个简单安全的方法,并且可以有效降低术后复发率,延长病人生存时间。但是由于本研究是一个回顾性研究,录入病例数目较少,故结论的可靠性尚待进一步前瞻性随机对照研究加以验证。
参考文献
1. Shimada K, Sakamoto Y, Esaki M, et al. Analysis of prognostic factors affecting survival after initial recurrence and reatment efficacy for recurrence in patients undergoing potentially curative hepatectomy for hepatocellular carcinoma. Ann Surg Oncol. 2007; 14(8): 2337-47.
2. Sugimachi K, Maehara S, Tanaka S, et al. Repeat hepatectomy is the most useful treatment for recurrent hepatocellular carcinoma. J Hepatobiliary Pancreat Surg. 2001; 8(5): 410-6
3. Tai A, Erickson B, Khater KA, et al. Estimate of radiobiologic parameters from clinical data for biologically based treatment planning for liver irradiation. Int J Radiat Oncol Biol Phys. 2008; 70(3): 900-7
4. Zhao JD, Xu ZY, Zhu J, et al. Application of active breathing control in 3-dimensional conformal radiation therapy for hepatocellular carcinoma: the feasibility and benefit. Radiother Oncol. 2008; 87(3): 439-44.
5. Zeng ZC, Tang ZY, Fan J, et al. Consideration of role of radiotherapy for lymph node metastases in patients with HCC: retrospective analysis for prognostic factors from 125 patients. Int J Radiat Oncol Biol Phys. 2005; 63(4): 1067-76.
6. Zeng ZC, Tang ZY, et al. Radiation therapy for adrenal gland metastases from hepatocellular carcinoma. Jpn J Clin Oncol. 2005 ; 35(2): 61-7.
7. Kumamoto T, Tanaka K, Matsuo K, et al. Adjuvant hepatic arterial infusion chemotherapy with 5-Fluorouracil and interferon after curative resection of hepatocellular carcinoma: a preliminary report.Anticancer Res. 2013; 33(12): 5585-90.
8. Tanaka K, Yabushita Y, Nakagawa K, et al. Debulking surgery followed by intraarterial 5-fluorouracil chemotherapy plus
9. subcutaneous interferon alfa for massive hepatocellular carcinoma with multiple intrahepatic metastases: a pilot study. Eur J Surg Oncol. 2013; 39(12): 1364-70.
10. Afdhal NH, Dusheiko GM, Giannini EG, et al. Eltrombopag increases platelet numbers in thrombocytopenic patients with HCV infection and cirrhosis, allowing for effective antiviral therapy. Gastroenterology. 2014; 146(2): 442-52.
11. Song do S, Bae SH, Song MJ, et al. Hepatic arterial infusion chemotherapy in hepatocellular carcinoma with portal vein tumor thrombosis. World J Gastroenterol. 2013; 19(29): 4679-88.
12. Hickey R, Vouche M, Sze DY, et al. Cancer concepts and principles: primer for the interventional oncologist-part II. J Vasc Interv Radiol. 2013; 24(8): 1167-88.
13. Mamada Y, Tajiri T, Akimaru K, et al. Long-term prognosis after arterio-portal embolization for hepatocellular carcinoma. Hepatogastroenterology. 2004; 51(55): 234-6.
14. Montorsi M, Santambrogio R, Bianchi P, et al. Survival and recurrences after hepatic resection or radiofrequency for hepatocellular carcinoma in cirrhotic patients: a multivariate analysis. J Gastrointest Surg. 2005;9(1): 62-67 .
15. Liang LJ, Hu WJ, Yin XY, et al. Adjuvant Intraportal Venous Chemotherapy for Patients with Hepatocellular Carcinoma and Portal Vein Tumor Thrombi Following Hepatectomy Plus Portal Thrombectomy. World J Surg 2008; 32: 627–631
16. Tan A, Aucejo F, Kim R. Is There a Role for Adjuvant Treatment after Hepatic Resection for Hepatocellular Carcinoma? Oncology 2010; 78: 161–171
17. Li Q, Wang J, Sun Y, et al. Postoperative Transhepatic Arterial Chemoembolization and Portal Vein Chemotherapy for Patients with Hepatocellular Carcinoma: A Randomized Study with 131 Cases. Dig Surg 2006; 23: 235–240
18. Chau GY, Liu WY, Tsay SH, et al. Postresectional Adjuvant Intraportal Chemotherapy in Patients with Hepatocellular Carcinoma: A Case-Control Study. Annals of Surgical Oncology 2006; 13(10): 1329–1337
19. 黎洪浩,区庆嘉,陈积圣,王捷. 肝癌根治性切除术后联合肝动脉化疗栓塞和门静脉化疗对预防复发的价值. 中华肿瘤杂志. 2000; 22(1):61-63
20. Huo TI, Lui WY, Wu JC, et al. Deterioration of hepatic functional reserve in patients with hepatocellular carcinoma after resection: incidence, risk factors, and association with intrahepatic tumor recurrence. World J Surg. 2004; 28(3): 258-62.
21. Katagiri S, Yamamoto M. Multidisciplinary treatments for hepatocellular carcinoma with major portal vein tumor thrombus. Surg Today. 2014; 44(2): 219-26.
22. Kim do Y, Han KH. How to improve treatment outcomes for hepatocellular carcinoma of intermediate and advanced stage. Dig Dis. 2012; 30(6): 598-602.
23. He Q, Kuang AR, Guan YS, et al. Puncture injection of para-toluenesulfonamide combined with chemoembolization for advanced hepatocellular carcinoma. World J Gastroenterol. 2012; 18(46): 6861-4.
24. Baek YH, Kim KT, Lee SW, et al. Efficacy of hepatic arterial infusion chemotherapy in advanced hepatocellular carcinoma. World J Gastroenterol. 2012; 18(26): 3426-34.
25. Ueda H, Fukuchi H, Tanaka C. Toxicity and efficacy of hepatic arterial infusion chemotherapy for advanced hepatocellular carcinoma. Oncol Lett. 2012; 3(2): 259-263.
26. Lee SS, Shin HS, Kim HJ, et al. Analysis of prognostic factors and 5-year survival rate in patients with hepatocellular carcinoma: a single-center experience. Korean J Hepatol. 2012; 18(1): 48-55.
27. Kneuertz PJ, Demirjian A, Firoozmand A, et al. Diffuse infiltrative hepatocellular carcinoma: assessment of presentation,
28. treatment, and outcomes. Ann Surg Oncol. 2012; 19(9): 2897-907.
29. Chen YY, Yen HH, Chou KC, et al. Thalidomide-based multidisciplinary treatment for patients with advanced hepatocellular carcinoma: a retrospective analysis. World J Gastroenterol. 2012; 18(5): 466-71.
30. Cui L, Liu XX, Jiang Y, et al. Comparative study on transcatheter arterial chemoembolization, portal vein embolization and
31. high intensity focused ultrasound sequential therapy for patients. Asian Pac J Cancer Prev. 2012; 13(12): 6257-61.
32. Liu L, Miao R, Yang H, et al. Prognostic factors after liver resection for hepatocellular carcinoma: a single-center experience from China. Am J Surg. 2012; 203(6): 741-50.
33. Kim do Y, Ahn SH, Kim SU, et al. Adjuvant hepatic arterial infusional chemotherapy with 5-fluorouracil and cisplatin after curative resection of hepatocellular carcinoma. Oncology. 2011; 81(3-4): 184-91.
34. Kolarević D, Tomasević Z, Boricić I. Metastasis of hepatocellular carcinoma presented as a tumor of the maxillary sinus and retrobulbar tumor. Vojnosanit Pregl. 2011; 68(4): 359-62.
35. Zhang ZM, Guo JX, Zhang ZC, et al. Therapeutic options for intermediate-advanced hepatocellular carcinoma. World J Gastroenterol. 2011; 17(13): 1685-9.
上一篇:曾宗渊 教授 主任医师
下一篇:钱伟 胸心外科 医学博士
相关热门词:











































 粤公网安备 44010602001792号
粤公网安备 44010602001792号